By Andrew Burchell, Research Fellow, Department of History
Founded in 1981 by the anthropologist David Pocock and the archivist Dorothy Sheridan at the University of Sussex, the Mass Observation Project (or MOP, for short) is a revival of the older Mass-Observation initiative (active 1937-c.1948). As with its predecessor, MOP recruits a national panel of ‘observers’ or ‘correspondents’ to send written responses to open-ended questionnaires (known as ‘directives’) on a variety of topics. (You can find a list of all directive topics since 1981 here.)
MOP aims to provide a record of ‘everyday life’ in Britain. It therefore tells us much about the NHS’s centrality to the nation that no fewer than four directives directly dealing with the service have been sent out since the project began: Directive (D) 15 in 1984, D50 in 1997, D82 in 2008 and D112 in 2018. Meanwhile, a wealth of material relating to the NHS lies buried in individual responses to other directives on connected topics such as illness, ageing, dementia and issues of general well-being.
MOP offers rich evidence of changing views across time, and its directives allow us to access voices from a range of generations; including those born before and after the ‘appointed day’ in 1948. The focus of this blog post are the 1997 and 2008 directives – sent out during anniversary years for the service – and the shifting position of the general practitioner (GP) within the health service. How observers wrote about GPs highlights both changes and continuities across generations.
The material reproduced from the Mass Observation Archive is copyright of the Mass Observation Archive Trust, University of Sussex. To reuse this material please get in touch with the Mass Observation Archive: www.massobs.org.uk.
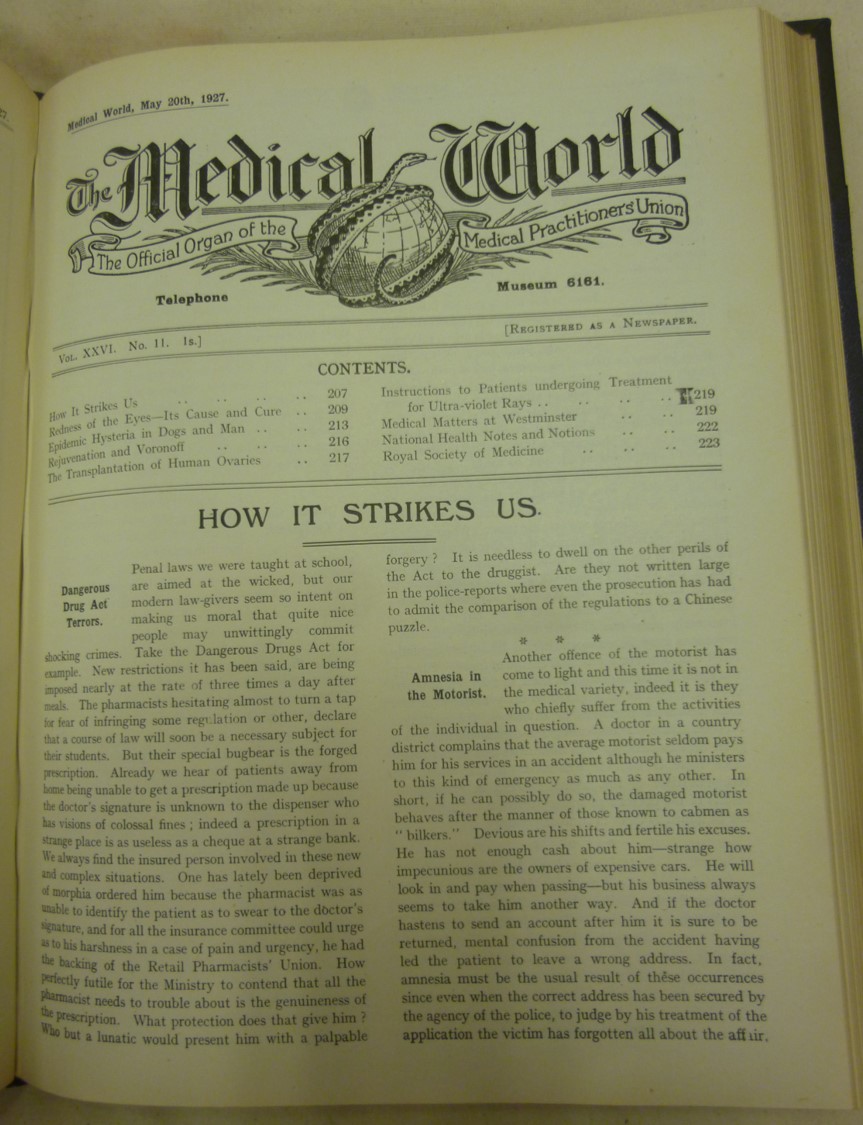
Medical World journal edition, 24 March 1933 [Modern Records Centre, MSS.79/MPU/4/1/16]
Medical World was the official publication of the Medical Practitioners’ Union (MPU), an organisation that split from the British Medical Association in 1914 and sought to promote increased state-involvement in healthcare. The MPU membership was heavily orientated towards general practitioners in the employment of the National Health Insurance system, including many of the pre-NHS ‘panel’ doctors recalled by older MOP respondents in 1997. It argued throughout the inter-war years, and during the 1940s negotiations over the creation of the NHS, for the family GP to have a significant role in the delivery of healthcare (often clashing with, and critiquing, local Medical Officers of Health). It merged with the Association of Scientific, Technical and Managerial Staffs in the 1970s and is today part of the wider Unite union.
Image reproduced from the Modern Records Centre with kind permission of Unite the Union.
GPs are, for many of us, our first point of entry into the services and care offered by the NHS. Yet their role was not always so strong, and their position owes much to the creation of the service and the important place that it afforded them in the delivery of healthcare. Indeed, the Royal College of General Practitioners was only founded in 1952, making it younger even than the NHS itself! Within that context, generation and age among the population as a whole govern relationships and attitudes, from those who first experienced GP care as children with the coming of the NHS, to those accessing care independently as teenagers or young adults in the 1980s and 1990s. A female observer (b.1965) writing in 1997 (when she would have been around 32) hinted at generational shifts in attitudes towards the GP. Whereas general practitioners were ‘once treated with reverence’ by patients like her grandmother, she argued, ‘we, in the younger generations’ perhaps risked being ‘too critical at times, but I do strongly believe we can improve health care’ (A2801, D50). Another female observer, in a similar age range, likewise contrasted her grandmother’s way of referring to the GP ‘in quite awesome tones’ to her own GP whom ‘I like … so much’ because ‘she seems so human!’ (D2239, b.1961, D50).
GP practices were themselves at the forefront of a series of policy and practice reorganisations within the NHS around the time of D50 and D82. GPs were moving into larger, shared surgeries, and technology (the increasingly ubiquitous computer) became part of consultations (see this 2002 piece in the BMJ on the enthusiastic uptake of computers by GPs). Older and younger respondents reacted to these shifts differently. A 1997 respondent in her forties felt that modern doctors were ‘more human’ and ‘no longer always claim to have all the answers’ – although she acknowledged that this could be ‘as frustrating and worrying’ as it could be comforting and helpful (B2728, female, b.1955, D50). Meanwhile, patients who would have been relatively young (or middle-aged) in 1997 were often entering middle-age (or early old-age) in 2008 and tended to feel that the rise of technology had aggravated a decline in doctor-patient relations. ‘I hate the way doctors sit and read the computer screen instead of … giving me their attention’, wrote a forceful K798 (female, b.1950, D82). For many of these respondents, fond memories of much older GPs were replaced by ‘[n]ew, young doctors in our local G.P. surgery’ who ‘seem to lack compassion and sympathy for their surroundings’ (R860, female, b.1947, D82), with ‘the rapport you once had with a family doctor now replaced by a harassed panel of bureaucrats’ (A4127, male, b.1962, D82). The ageing process had inverted the doctor-patient relationship: comforting childhood memories of an impressive, older doctor – who, in reality, might have only been in their mid/late-thirties but seemed older from the perspective of a child – had been replaced by the reality of treatment by someone potentially young enough to be a child or grandchild.
Frequent changes among GPs (a by-product both of rising professional stress and the health centre/practice model) also drew criticism among younger and older patients alike, and there was a feeling that this had led to GPs being more distant (C3210, female, b.1980, D82) – although some younger participants felt that these larger practices offered more options, particularly for young female patients who wanted to see a doctor of the same gender (C4131, female, b.1982, D82). This is a testament both to expanding representation of women (and also ethnic minority groups) among GPs, and it suggests that a desire to access doctors with similar gender or other characteristics to the patient (and therefore more understanding) may have become a generational dividing line for younger respondents. Older observers, meanwhile, grounded their criticisms in a story of decline over time: a perceived shift away from GPs ‘interested in the whole person’ towards simply ‘treat[ing] symptoms and provid[ing] pills’ (M3085, male, b.1949, D82). Of course, GPs themselves also feared this trend – but it is revealing that such medical opposition to diagnosis-by-computer and treatment-by-pill was largely invisible to the MOP writers, leading many to see the profession’s position in abstract, absolute terms.
Alongside GP reorganisation, respondents offered opinions on a concurrent new development in the 1990s and 2000s: the rise of patient ‘choice’. One of the elderly respondents in 2008 wrote scathingly that she did not ‘like being given choices when my GP obviously knows more than I do!’ (R2144, female, b.1935, D82). Phrases such as these demonstrate that the agenda of patient ‘choice’ was not always experienced as empowering for those more accustomed to accept medical advice unquestioningly. The obverse of this is reflected in the views articulated by the small number of GPs writing for MOP: ‘What I don’t like is the assumption that I am a baddie and that if people are kept waiting it’s because of laziness or some kind of incompetence on my part’, wrote B2623 (female, b.1944, D50). That professionals felt the need to be so defensive of their position highlights the shift in the wider popular perception of the doctor, away from infallibility towards critique.
It is very difficult to pinpoint exactly when the transition between different generations within respect to NHS attitudes occurs, and it may well be bound up with many things, including the rise of patient consumer groups and activism. It is also the product of wider narrative shifts in popular culture which have imbued the NHS with a unique creation story and put it in a prominent place within the national psyche. Yet it is revealing that the respondents born several decades after Nye Bevan’s ‘appointed day’, although taking the NHS for granted, often found it difficult to frame the service in the abstract, instead atomising it to the level of individual practitioners. One 38-year-old observer in 2008, for example, felt unable to ‘talk about a relationship with the NHS, as though it’s a brand like Tesco. It’s more a case of coming across individual health care practitioners’ (H4235, male, b.1970, D82); while a twenty-one-year-old observer responding in 1997 noted: ‘When looking at the questions on the directive, I was trying to work out why I didn’t really seem to have any particular views on the NHS. I think this is probably because as a child I spent so much time being ill, being visited by doctors, and visiting them, and going to hospital that the NHS became something that “just was”’ (W2782, female, b.1976, D50).

This image is taken from a page on the current NHS website, promoting the GP service and careers in it.
Note the increased presence of digital technologies – something commented upon, not always positively, by the MOP respondents.
That ‘just being’ of the NHS may now be altering, with the rise of what appear as ‘new threats’ to the service – and a new generation of activists against privatisation. The figure of the general practitioner remembered by so many of the MOP respondents was a key component of this background ubiquity. Yet it was a ubiquity which intersected with broader issues around medical authority and who was perceived to possess it. It was also an image that evolved across generations and was rooted in the reflexive process of ageing; as older observers compared their GPs in the present with the GPs of their youth, and as observers of a variety of ages navigated the changes being wrought to the NHS in the 1990s and 2000s.
The cover image for this blog post is from Jean Mohr and John Berger, A Fortunate Man: the story of a country doctor (Edinburgh: Canongate, 2017 [original publication: Allen Lane, 1967])
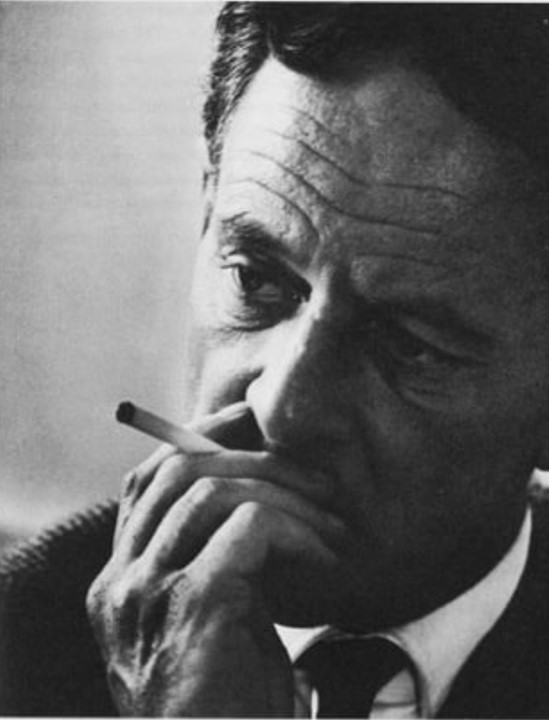
Image reproduced with kind permission of the rights holders and Canongate Books.
Copyright © 1967 by John Berger. Copyright renewed 1995 by John Berger.
Photographs copyright © 1967 by Jean Mohr. Photographs copyright renewed 1995 by Jean Mohr.
A Fortunate Man was the result of a collaboration between the British author and broadcaster, John Berger (1926-2017), and the Swiss photographer Jean Mohr (1925-2018). Mohr had a career documenting humanitarian and refugee aid. Berger had recently relocated to the Forest of Dean, befriending his local GP, identified in the book as ‘John Sassall’ (Dr John Eskell).
Part social reportage, medical biography and meditation on the place of the GP within a nationalised healthcare system, A Fortunate Man presents a different, more personal, perspective on the NHS GP. (Not least a GP with a cigarette!)

Image reproduced with kind permission of the rights holders and Canongate Books.
Copyright © 1967 by John Berger. Copyright renewed 1995 by John Berger.
Photographs copyright © 1967 by Jean Mohr. Photographs copyright renewed 1995 by Jean Mohr.
In A Fortunate Man, Sassall emerges as a human being with his own concerns and anxieties for his patients in a working-class rural community rather than an objectively removed scientist. This exerted an impact on his own health and psychological state. He committed suicide in 1982. Berger writes of his GP subject: ‘He was scarcely ever in the surgery. He imagined himself as a sort of mobile one-man hospital’ (p. 56). Although in many respects a maverick, the ‘Sassall’ variety of GP (active within the local community) was recalled with fondness by several MOP respondents from older generations.
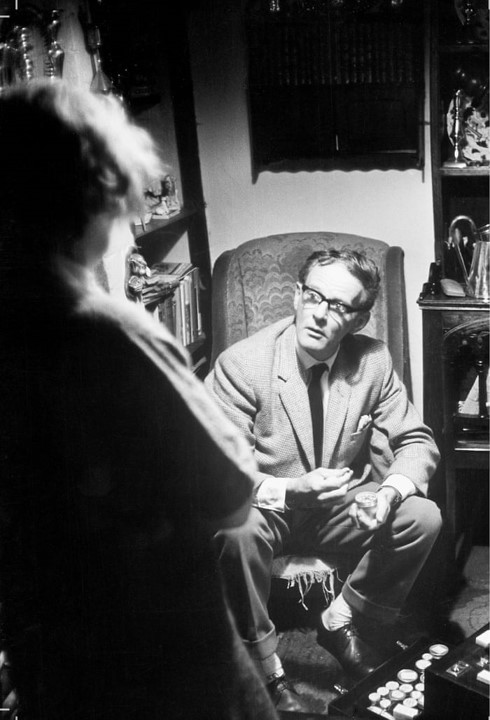
Image reproduced with kind permission of the rights holders and Canongate Books.
Copyright © 1967 by John Berger. Copyright renewed 1995 by John Berger.
Photographs copyright © 1967 by Jean Mohr. Photographs copyright renewed 1995 by Jean Mohr
Note how, in the composition of this picture, the GP is the focal point. The ‘patient’ is an indistinct, standing figure in the foreground with their back to the spectator, while the line of vision looks down (from over the patient’s shoulder) onto the GP sat in an armchair.
The material reproduced from the Mass Observation Archive is copyright of the Mass Observation Archive Trust, University of Sussex. To reuse this material please get in touch with the Mass Observation Archive: www.massobs.org.uk.


